What does the term polypectomy refer to?
Polypectomy refers to the removal of colon polyps during colonoscopy. It has been established that polypectomy decreases the risk for colorectal cancer.
How are colon polyps removed?
The polyps are removed during colonoscopy with a variety of techniques depending on polyp size, shape and location (Figures 1-4). During the procedure the patient remains sedated and experiences no pain or discomfort.



Are there any polypectomy-related complications?
Endoscopic polypectomy is definitely a safe procedure. Its most common complications are bleeding and perforation, occurring in approximately 1 in 1000 patients. Bleeding can be stopped immediately with hemostatic methods including application of clips, adrenaline injection and coagulation. Perforation may be managed either conservatively with intravenous fluids and antibiotics or surgically, taking into account several factors.
Should the endoscopist be aware of my medications prior to polypectomy?
Anticoagulants, antiplatelets and anti-inflammatory drugs are of special interest. The gastroenterologist may also ask for blood tests prior to the procedure or even discuss with other doctors (e.g. cardiologists) regarding coagulation issues for each individual patient.
What happens after I have polyps removed?
In the vast majority of cases the patient returns back home and their everyday activities after polypectomy. You might need to have a colonoscopy every few years to look for new polyps. Also, if the polyps you had removed were of the precancerous type, people in your family might need to be checked for polyps and colon cancer, too.
What does the term Endoscopic Retrograde Cholangiopancreatography (ERCP) refer to?
ERCP is an examination used for the diagnosis and treatment of biliary and pancreatic diseases. It has been developed in the 1980’s and has dramatically decreased the need for major open surgical interventions.
How is it performed;
During ERCP the patient remains under deep sedation and feels no pain or discomfort. The endoscope is advanced through the mouth, esophagus and stomach into the duodenum and reaches an area called ampulla of Vater, where both bile and pancreatic ducts drain (Figure 1). A small plastic tube (cannula) is passed through the endoscope into the opening of the bile duct, dye is injected, and X-ray pictures are taken. Subsequently, a small cut in the duodenal wall is made so that the endoscopist can perform a variety of therapeutic interventions (stone extraction, stent placement etc.) according to the diagnosis (Figure 2).


ERCP indications
- Obstructive jaundice
- Choledocholithiasis (stones in common bile duct)
- Malignancies of the pancreas or biliary tract (cytology and stent placement)
- Benign biliary strictures
- Acute lithiasic pancreatitis (with co-existing cholangitis)
- Biliary tract trauma (iatrogenic or not)
Are there any complications?
ERCP can be accompanied by complications like pancreatitis, bleeding and perforation, the two latter being extremely rare (<1%). Pancreatitis (inflammation of the pancreas) is the most frequent complication, occurring in about 5 to 7 percent of people undergoing ERCP. When it occurs, it is usually mild, causing abdominal pain and nausea, which resolve after a few days in the hospital. Rarely pancreatitis may be more severe.
A variety of endoscopic and pharmaceutical methods exist to decrease the incidence of post-ERCP pancreatitis. Mandatory parameters include careful patient selection and an adequately trained endoscopist. In the USA training in ERCP is provided additionally to the standard gastroenterology program (i.e. fellowship in advanced endoscopy). Dr. Scotiniotis has received such training in the University of Pennsylvania, Philadelphia, while Dr. Sioulas has obtained a similar experience in the University Hospital of Hamburg, Germany.
What is Endoscopic Ultrasound (EUS)?
ΕUS is an examination that combines endoscopy and ultrasound. In that way we are able to examine deeper parts of the esophageal, gastric or bowel wall as well as the surrounding tissues (mediastinum, pancreas, biliary system, lymph nodes, etc.).
How is it performed?
The patient is under sedation and feels no pain or discomfort. The procedure is accomplished with a specialized flexible endoscope and lasts approximately 30 minutes. Afterwards, the patient returns home.
What are the indications for EUS?
- Diseases of the pancreas and biliary tract:
EUS enables detailed examination of the pancreas and extrahepatic biliary tract. It may clarify lesions that are found in other examinations like CT and MRI or even diagnose extremely small lesions (sized 5-10mm) that can not be identified otherwise (Figure 1). It is also very useful for the assessment of pancreatic cystic lesions.

-
Staging of esophageal, gastric and rectal cancer:
EUS is a very precise tool for the staging of esophageal, gastric and rectal cancer. Furthermore, in the preoperative setting EUS can identify those patients that are eligible for neoadjuvant chemotherapy (i.e. chemotherapy prior to surgery). -
Submucosal lesions of the gastrointestinal wall:
EUS enables examination of the deeper layers of the gastrointestinal wall. Accordingly, submucosal lesions can be assessed to guide further management. Surrounding tissues and vessels (e.g.varices) can be also evaluated.What is EUS-FNA?
EUS-guided Fine Needle Aspiration (EUS-FNA) is the acquisition of tissue from tumors or fluid from cysts through thin needles under EUS guidance. It has been shown that EUS-FNA contributes significantly in the diagnosis of various abdominal masses and the correct characterization of cysts (e.g. pancreatic cysts) (Figure 2).



A few EUS-FNA performing centers exist in our country. Our experience involves more than 1500 patients referred to us from all over Greece. The examination is painless and extremely safe (pancreatitis in only 0.6% of the cases). According to the results of internal audit our sensitivity for diagnosing malignancy reaches 95%, being within the recommended international standards.
What does the term stents refer to?
A stent is a small mesh tube that is used to open narrowed regions in the gastrointestinal tract. Stents are placed endoscopically during gastroscopy, colonoscopy or ERCP, depending on the position of the narrowing.
What are the available stent types?
Two types of stent exist: plastic and metal. The gastroenterologist selects the appropriate type according to the lesion.
What are the indications for stent placement in gastrointestinal diseases?
Stents are indicated for a variety of benign and malignant lesions of the gastrointestinal tract (including the bile duct). They aim to provide relief from obstructive symptoms such as difficulty swallowing, pain, vomiting, and jaundice (Figures 1, 2).
Our team performs stent placement for all indications and is also one of the first to apply EUS (endoscopic ultrasound) – guided stent placement for drainage of pancreatic pseudocysts in Greece (Figure 3).



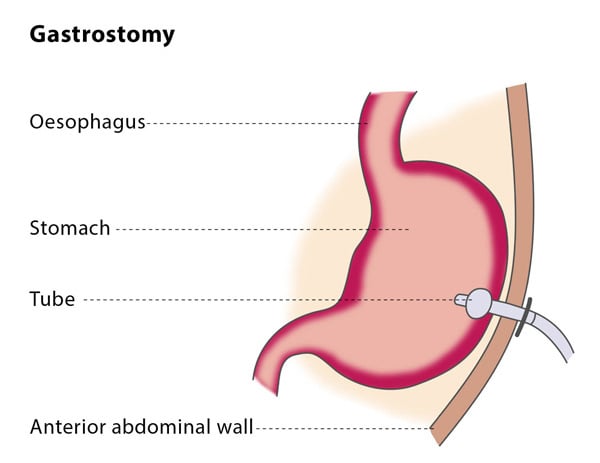
What does percutaneous endoscopic gestrostomy (PEG) refer to;
It refers to the endoscopic placement of a thin feeding tube that comes out from the stomach and through the abdominal wall (Figure ).
Which patients need PEG;
It is very helpful for patients who are not able to be fed properly by mouth. Examples are those suffering from dementia, Parkinson’s disease, obstructing upper gastrointestinal or airway malignancies, and trauma patients. It is also indicated for cancer patients who are planned for radiotherapy in order to prevent treatment-related feeding problems.
Describe the preparation and the procedure for PEG placement
The patient should be fasting for the previous 6 hours. Anticoagulants and antiplatelet drugs have to be withdrawn. Prophylactic antibiotics are given prior to the procedure. During the intervention the patient remains deeply sedated and has no pain or discomfort. The total duration of the procedure lasts no longer than 15 minutes.
What follows PEG placement?
Feeding is initiated through the gastrostomy tube approximately 12 hours after placement. Detailed instructions regarding routine gastrostomy tube care are given to the patient’s caregivers. A normal diet can generally be followed, given in several small meals during the day. Six months after placement, the patient has to return for a hospital visit in order for the tube to be replaced. Subsequent tube replacements can be carried out at home.